Maureen Burger (mburger@visanteinc.com) is Chief Nursing Officer for Visante Inc. living in Indianapolis, IN.
Drug diversion didn’t disappear when COVID-19 patients arrived at your hospital in 2020. Many changes associated with managing the COVID-19 pandemic in hospitals may in fact be creating new opportunities for drug diversion that could be difficult to detect if you don’t know what you are looking for. Because of the immediate needs to increase capacity to care for COVID-19 patients, prevent exposure, and to preserve personal protective equipment (PPE), the Drug Enforcement Administration (DEA) allowed several changes that “loosen” requirements for chain of custody. In addition, hospitals have implemented workflow changes to facilitate care that may also facilitate drug diversion. It is difficult to predict if and when the COVID-19 pandemic will be controlled, and the combination of the 2020 flu season with persistent COVID-19 may extend the new normal for hospital operations. This article will outline some of the COVID-19 changes and introduce a new model, the Drug Diversion Triad, to demonstrate the impact of COVID-19 on drug diversion in US hospitals.
What has DEA changed?
DEA recognized that the current regulations for controlled substances may need to be adjusted to prevent unnecessary exposure to persons and to maintain the continuum of care for patients. A series of exceptions was granted to facilitate both inpatient and outpatient care, beginning in March 2020, extending until the public health crisis is ended.
Telemedicine
Healthcare providers across the US shifted away from face-to-face patient encounters and began to rely on telemedicine/remote patient visits. Many states waived the individual state medical license requirements and granted reciprocity to adjacent states in order for practitioners in one state to prescribe medications, including controlled substances, to patients in a reciprocal state. Typically, DEA would require a separate DEA registration in each state where the practitioner would prescribe, dispense, and administer controlled substances. Due to the extraordinary circumstances posed by COVID-19, DEA waived this requirement as long as the practitioner has a DEA registration in one state and has permission under another state where the controlled substance dispensing occurs.[1] Anytime there is a public emergency and an increase in demand for practitioners, hospitals may use an expedited process to verify practitioner credentials. The unique circumstances posed by interstate telehealth visits could potentially be used as a novel way to increase controlled substance prescribing with the intent to sell to persons who are unable to fill the need for either licit or illicit drugs.
Registration
Some hospitals and clinics had the need to set up additional spaces to care for COVID-19 patients. The temporary spaces are not at the same location as the registered site. Normally a DEA registration is required for every separate address/location. To facilitate opening the overflow sites, DEA permitted the hospitals to add the satellite locations to their existing registrations. In addition, DEA permitted distributors to directly ship controlled substances to the nonregistered satellite locations.[2] This change, along with permitting a fax/scanned copy of a DEA Form 222,[3] creates a potential opportunity to send an illicit order and accept delivery before diversion is detected.
Form 222
While the majority of Schedule II drugs are ordered using the Controlled Substance Ordering System, when an organization uses DEA Form 222, the purchaser is required to mail the original form to the distributor and retain a copy. Sending the purchase order by mail during the pandemic could potentially affect the supply of controlled substances needed to care for patients during this time of unusual demand. DEA granted an exception to permit the purchaser to fax or scan Form 222 to the distributor until the public emergency is ended. Following the return to normal business, the purchaser must send the originals to the distributors. Relaxing this requirement would make it easier to send a tampered/illicit order for controlled substances, with delayed detectability of ordering and receipt, especially if delivered to an off-site, nonregistered location.
5% rule
Hospitals are registered with DEA as practitioners and are permitted to “dispense,” and may also “distribute,” a limited amount of controlled substances to another practitioner (e.g., a hospital, pharmacy, or other practitioner).[4] The requirements limit the practitioner from distributing more than 5% of the total number of dosage units of all controlled substances that the hospital dispenses and distributes during that year. DEA has granted an exception to the 5% rule for hospitals so that they can ensure the supply of controlled substances to patients without having to become registered as a distributor.[5] While the relaxation in the 5% rule has facilitated movement of controlled substances in order to meet patient care needs, it may lessen the detectability of illicit requests for controlled drugs.
Distributors
Hospitals may not want to have controlled substances delivered to the usual address/location at a registered site/address to prevent exposure to COVID-19. DEA will allow a distributor to deliver to a “safe zone” designated by the registrant if the delivery is made directly to a person/agent of the hospital.[6] The delivery may not be left for pickup at later time, only given directly to another person. A savvy employee intent on bulk diversion could foreseeably submit an illicit Form 222 and take delivery within a designated safe zone without detection.
What have hospitals changed?
Hospitals have had to find creative solutions to meet the needs of the patients and healthcare providers in order to conserve staff, reduce the risk of exposure, and preserve PPE. Pharmacy staff are limited in their ability to deliver into units caring for COVID-19 patients. Nurses are limited in their ability to access both drugs and their patients because of restrictions on PPE use. Here are some of the novel approaches hospitals are using that may increase access of staff to controlled substances and opportunities for drug diversion.
Elimination of BioID for automated dispensing cabinets
Healthcare workers in a COVID-19 unit may be required to wear PPE, including gloves, at all times. This would include when removing drugs from an automated dispensing cabinet. Gloves interfere with the fingerprint scanner used for BioID, so the hospital may deactivate this function and require a username and password for secured access. The drawback of this approach is the sharing of username/password combinations to remove drugs for coworkers and potentially misidentified controlled substance transactions.[7]
Unsecured pneumatic tube system
Caring for COVID-19 patients who require mechanical ventilation has caused a massive increase in the use of controlled substances, especially for continuous infusions. Some hospitals began stocking compounded controlled substance infusions in the automated dispensing systems, and some hospitals may be delivering infusion bags via pneumatic tube system. Not all tube systems are set up to maintain the chain of custody for controlled substances. The tube system needs to be in a location of continuous observation and should have secured doors that only unlock with a valid passcode of a swipe card. Hospitals without security features are at risk for undetected loss when the carrier arrives and a drug is removed by an unauthorized person. This creates an opportunity for both tampering and/or theft. Large-volume infusions would need to be stored in automated dispensing towers versus drawers, thus increasing access for tampering or theft.
Temporary units/temporary staff
A few hospitals in major metropolitan areas set up field hospitals in remote locations such as convention centers and parking lots. Many more hospitals set up temporary units within the hospital walls to care for the overflow of COVID-19 patients. Automated dispensing machines (ADMs) were deployed as part of the unit infrastructure. To meet the urgent needs and deliver service in a timely manner, the ADM systems may have been set up with a nonstandard configuration. Persons with the knowledge of ADM configurations would be able to exploit these differences and divert controlled substances.
Not all hospital staff are qualified to care for critically ill patients. So, while there are staff without work due to cancelled surgeries and procedures, there is a shortage of competent staff to care for COVID-19 patients. Temporary staff (physicians, nurses, pharmacists) are in high demand to fill the gap. The urgency of the situation plus the sheer volume of temporary staff led to expedited preemployment screening (background checks, preemployment drug testing) that may permit healthcare workers with controlled substance dependency into hospitals.
Human resource restrictions
The American Hospital Association estimates the total four-month (March 1–June 30, 2020) financial impact as $202.6 billion in losses for America’s hospitals and health systems, or an average of $50.7 billion per month.[8] The losses were driven in the most part by four factors:
-
Increased costs from caring for COVID-19 patients,
-
Decreased revenue from cancelled cases and procedures,
-
Increased costs associated with providing PPE, and
-
Increased costs to support healthcare workers.
Many hospitals have used rolling staff furloughs and/or layoffs to reduce expenses and slow their losses. In addition, many of the professionals assigned to provide oversight for drug diversion prevention, surveillance, and investigation are now working from home. Remote work prevents direct observation, making detection of anomalous behaviors more difficult.
Impact on our staff
The physical, emotional, and financial toll of COVID-19 on healthcare workers cannot be overstated. At the onset of the public health emergency, many workers were either sent home or redeployed to unfamiliar units to care for unfamiliar patients. Frontline workers experience anxiety, mistrust, fatigue, depression, insomnia, lingering physical ailments, anger over the lack of PPE, and fear that they will get COVID-19 or spread it to their families.[9] Financial uncertainty due to either personal lack of income or income loss from spouses and significant others is overwhelming. The loss of childcare services and added responsibility of homeschooling compound the stressors for healthcare workers.
Discussion
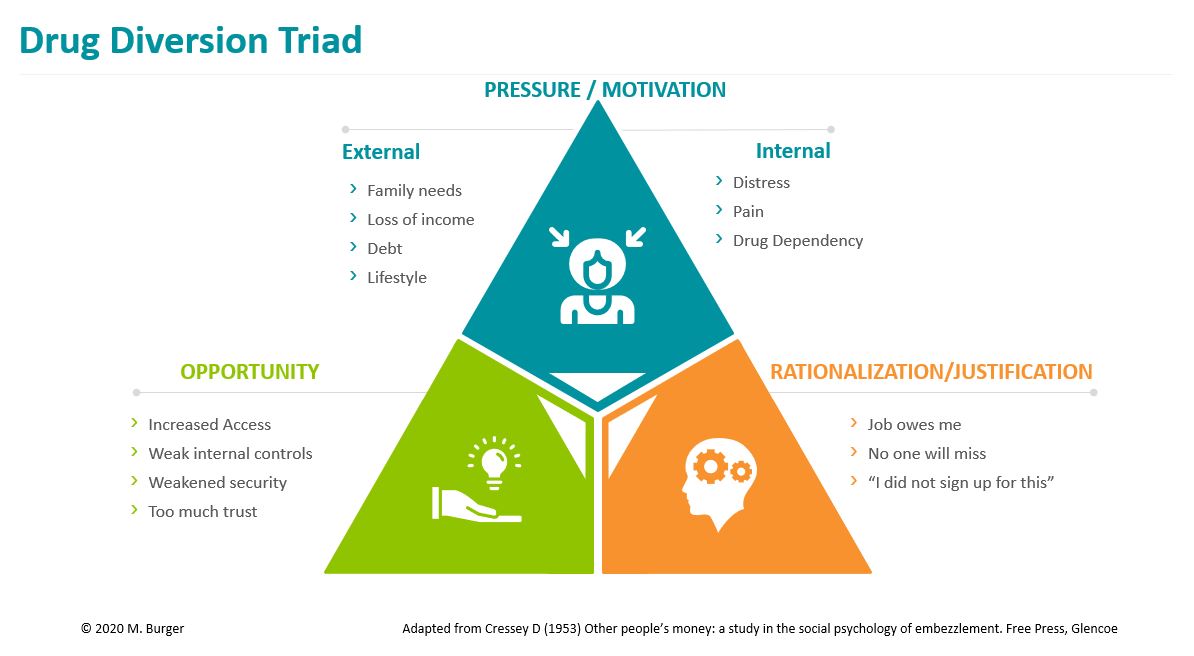
Healthcare facility drug diversion is similar to fraud, except the item of value is not money; it is controlled drugs. Organizations are faced with the complexity of trying to prevent, detect, and manage diversion events. It is helpful to examine drug diversion through the lens of Cressey’s fraud triangle, modified specifically as a Drug Diversion Triad (Figure 1), to better understand which factors present opportunities for intervention.
The fraud triangle was originally conceptualized by Donald Cressey in 1953[10] and has undergone adaptations over time. Essentially, all three parts of the triangle must exist before a person commits fraud. Drug diversion is a type of fraud, as the individual intends to deceive the organization for the purpose of personal benefit. All three elements need to be considered when assessing for risk of drug diversion.
Pressure/motivation
Motivation to commit drug diversion can be either external or internal. External factors could include family need, such as a family member with a chronic pain or substance use disorder needing drugs to avoid withdrawal. Another external source of motivation is loss of income: diversion for sale can make up a significant part of family income lost to unemployment during the pandemic. Rising debt from any source can be a potent pressure to divert drugs for sale. And finally, lifestyle choices may increase pressure to either divert for sale or personal use. All of these factors are difficult to detect and may be unknown to the organization.
Internal factors causing motivation to divert drugs can include mental distress, especially the additional stress induced by caring for patients during the pandemic, or physical pain from latent injuries or just getting overworked during the pandemic. Substance misuse in healthcare workers is difficult to detect and can develop following licit or illicit use of controlled drugs. While an organization may know when an employee is returning to work following time off for illness or injury, there is no way to know whether the individual had developed a dependency on prescribed controlled drugs or from illicitly obtained drugs. A healthcare worker with drug dependency could be consumed with finding a way to prevent withdrawal.
Rationalization/justification
Many healthcare organizations survey staff on a regular basis to determine their level of engagement and satisfaction. The results may help determine opportunities for leadership coaching of problem areas where staff are disgruntled in general, but they do not let you into the heads of the individuals. Unhappy, overworked, stressed-out staff may find justification for drug diversion when they feel underappreciated, undercompensated, and disenchanted with their work. COVID-19 pandemic conditions may be the last straw for some staff who just needed a little push to justify diverting drugs—either for sale or for personal use. Similar to motivation/pressure, it is not easy to detect how an individual can justify the act of drug diversion.
Opportunity
Finally, there is opportunity. How many times have you heard that a department/unit does not worry about drug diversion because they trust in each other? A successful drug diversion program cannot be built on trust; it is built on checks and balances. The access changes to automated dispensing machines, expanded individual access to enable staff to work on multiple units, lagging access deactivation, expanded storage of large-volume infusions of controlled drugs on patient care units, and less direct observation of staff are all ways to expand access to controlled drugs for both authorized and unauthorized staff. Hospitals that furlough nonessential workers or mandated remote work for nonpatient-care staff may suffer a loss of detection/surveillance of anomalous behavior with controlled drugs. New ways to deliver, store, and document chain of custody are being used to accommodate changes in care delivery, but without appropriate oversight, the diversion risks may go unnoticed.
The Drug Diversion Triad operates similarly to Cressey’s fraud triangle, where all three elements would be present and only opportunity is easily detectable. Opportunity is the only element where risk mitigation strategies may be successful. The hospital drug diversion program must not be put on the shelf during a pandemic, and diversion surveillance and detection should receive increased scrutiny.
If your organization has a formal drug diversion program, please check to see how the pandemic has affected the staffs’ ability to be present and strong. If your organization lacks this level of structure, you may consider posing this as a concern to the executives. Building awareness is the first step to gaining resources to ensure the organization will be compliant throughout the pandemic and after. The Drug Diversion Triad may be a good way to initiate dialogue about the increased risk of drug diversion during the COVID-19 pandemic.
Takeaways
-
Regulatory changes made during the COVID-19 pandemic can increase the risk of drug diversion in hospitals.
-
Changes in pharmacy and patient care policies to accommodate the pandemic create new and/or enhance existing opportunities to divert controlled drugs.
-
Oversight for drug diversion surveillance and detection may be reduced due to furloughs and remote work.
-
New pressures and justifications may be present in hospitals that care for COVID-19 patients.
-
The Drug Diversion Triad model may be useful to build awareness about increased risks of drug diversion.